DHCS on the Bold Goals: Equity Is Still the Point — the Question Is How
On February 5 of this year, 65 health care and community organization leaders from across California gathered in Oakland for the latest California Improvement Network (CIN) partner meeting. CIN supports health plans, providers, and community-based organizations to translate strategy into action. CIN fosters cross-sector problem-solving, sharing what’s working, and building relationships that drive durable improvement. For this meeting, one question anchored the day: What comes next for Medi-Cal quality efforts? Standing before the room, Pam Riley, chief health equity officer and assistant deputy director of quality and population health management at the California Department of Health Care Services (DHCS), set the tone.
“Let me say this clearly: Equity remains central to our work. The question isn’t if we continue the work — it’s how.”
The Bold Goals Were Never Simply About Metrics
Launched in 2022 as part of Medi-Cal’s Comprehensive Quality Strategy, the Bold Goals set an ambitious target to improve priority quality measures by 50% and close racial and ethnic disparities in three clinical areas by 2025. These goals reflect some of the most persistent gaps for Medi-Cal members: children’s preventive care, behavioral health, and maternal health and birth equity.
DHCS expects final 2025 results later this year; in the meantime, public dashboards show progress to date, not the full, final picture. Riley emphasized that the goals were intentionally ambitious and that transparency remains central, with ongoing updates available through the CalAIM dashboard.
The Bold Goals roll up performance on specific quality measures reported by Medi-Cal managed care plans through established quality reporting processes (including measures based on administrative and clinical data).
One of these measures is of well-child visits, which are preventative health exams that track growth, screen for health issues, and keep children up to date on vaccines. As of March 2026, the CalAIM dashboard shows the percentage of children that had at least six well-child visits in their first 15-30 months of life (denoted in the dashboard as W30-6+).
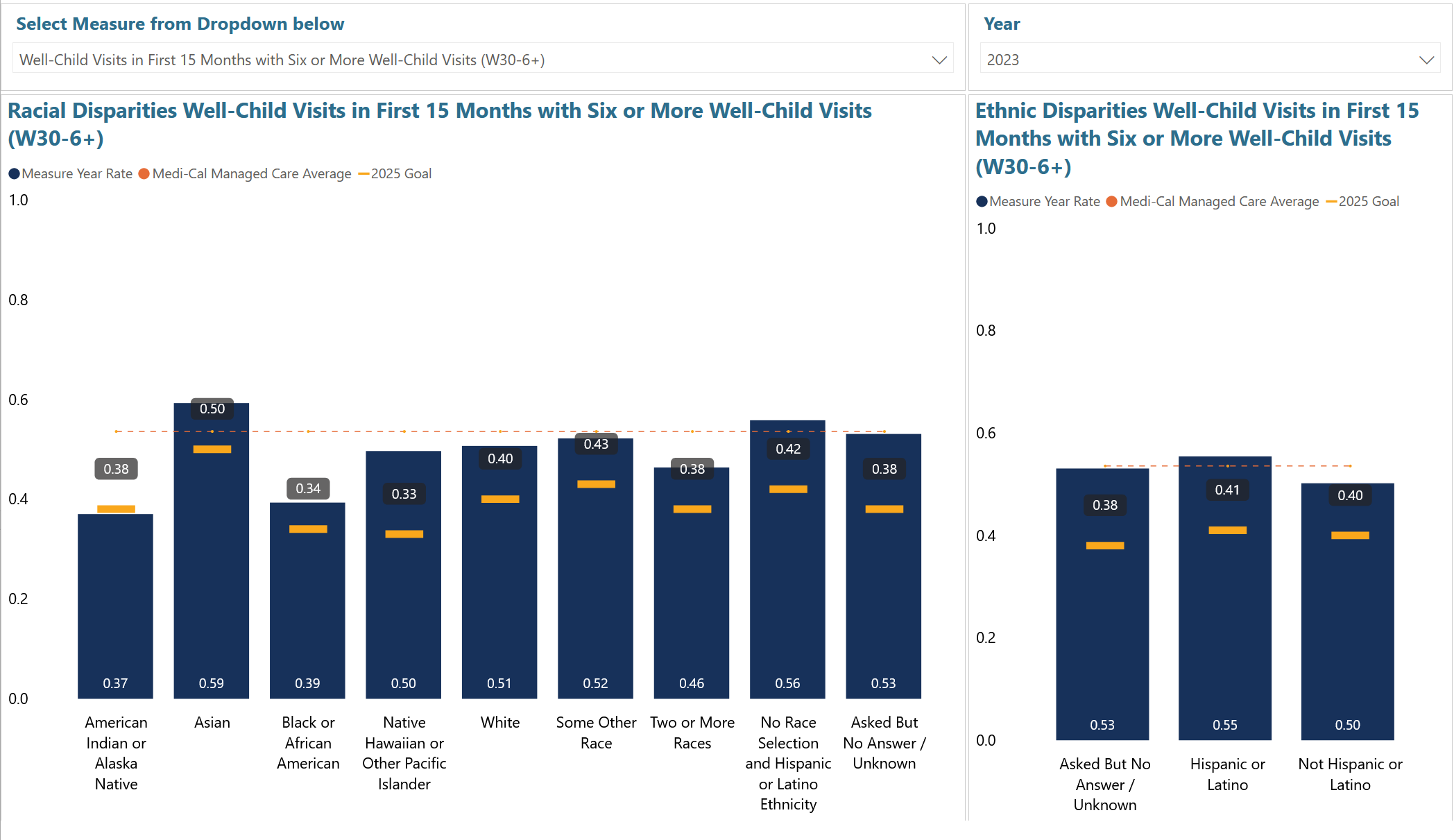
Results from 2023 from the CalAIM Dashboard on the Target to Close Racial and Ethnic Disparities in Well-Child Visits and Immunizations by 50%
While progress is meaningful, performance lagged in some communities. DHCS is seeing that pattern in the Bold Goals data, with disparities persisting in certain measures for Black and Indigenous Medi-Cal members and in particular geographic areas. While each ethnic group made some improvement, metrics for Black and Native Medi-Cal members didn’t improve as much as members of other races. That’s why Riley returned to a core premise that many CIN partners build into their improvement work: “There is no quality without equity.”
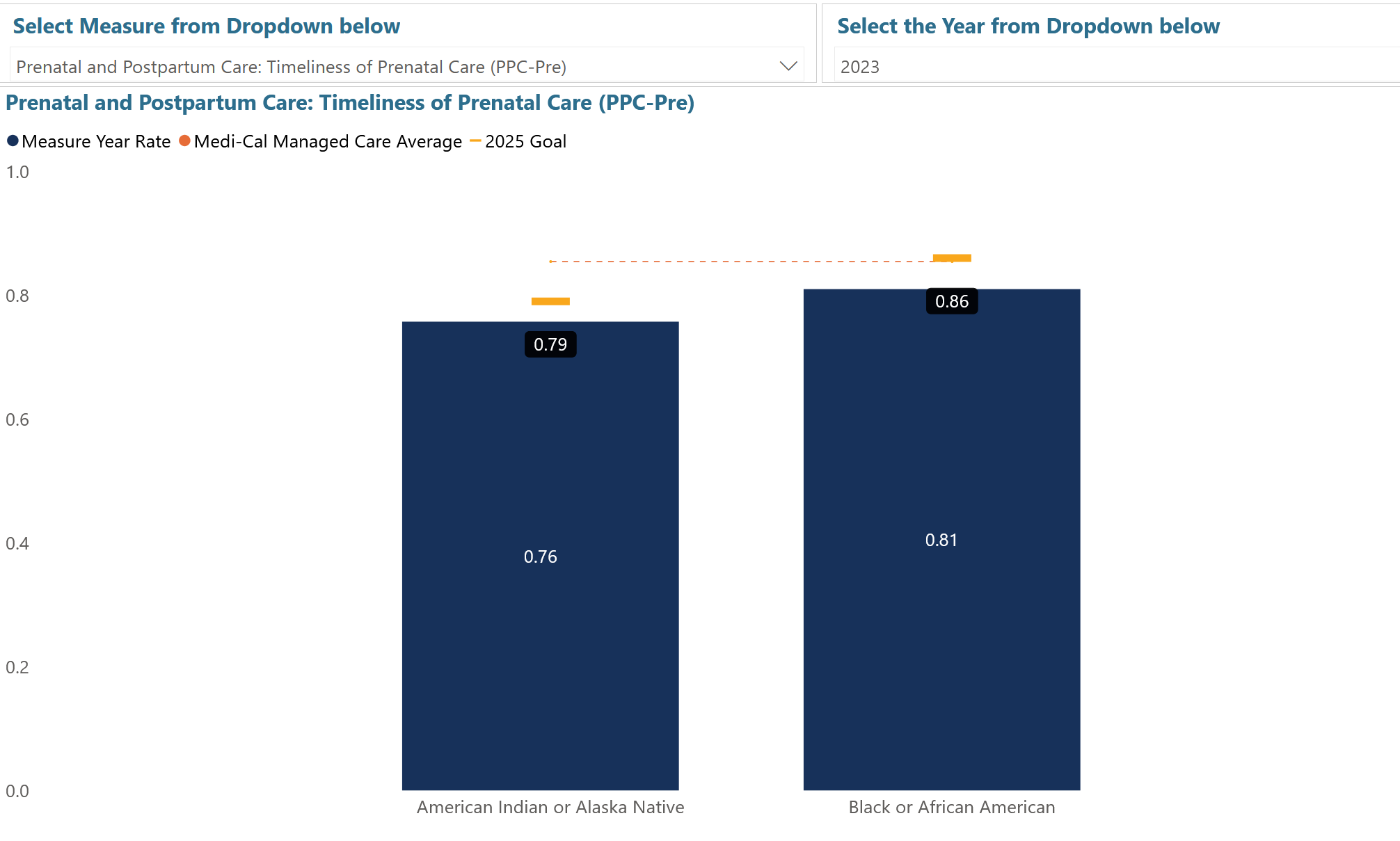
Results from 2023 from the CalAIM Dashboard on the Target to Close Maternity Care Disparities
For prenatal and post-partum care, these disparities continue. More details can be found in the CalAIM dashboard.
A Challenging Federal Context Makes the “How” More Urgent
Riley did not sidestep the broader environment. Potential federal Medicaid changes could increase the uninsured rate and strain already stretched systems. As coverage and funding become increasingly precarious, the work of equity-based care becomes harder to staff, harder to sustain, and harder to scale.
What DHCS Is Prioritizing Now
Even amid uncertainty, DHCS is continuing targeted initiatives aligned with the Bold Goals, including these:
- Child Health Strategy (2022). Launched in March 2022 to bring existing and new child and family initiatives under one umbrella, it aims to strengthen DHCS oversight and accountability for children’s services and to promote whole-child, preventive, family- and community-based care while reducing disparities.
- Birthing Care Pathway. The pathway is a DHCS road map developed beginning in 2023 to improve care for pregnant and postpartum Medi-Cal members from conception through 12 months postpartum, with explicit goals to reduce maternal morbidity and mortality and to address racial and ethnic disparities that disproportionately affect Black people, American Indian / Alaska Natives, and Pacific Islanders.
- Behavioral Health Transformation. CalAIM’s behavioral health reforms are designed to support integrated, whole-person care and reduce fragmentation by simplifying how Medi-Cal behavioral health is administered, alongside policy updates and payment reform that continue rolling out through 2027.
- CalAIM implementation. CalAIM is DHCS’s multiyear initiative to transform Medi-Cal through delivery system, program, and payment reforms, with goals that include addressing social drivers of health through whole-person approaches, reducing complexity for members, and improving quality outcomes while reducing health disparities.
Riley also outlined DHCS’s Health Equity Framework, which focuses on:
- Data collection and stratification
- Workforce diversity and cultural responsiveness
- Eliminating disparities through quality improvement
- Community and member engagement
That last pillar is where DHCS is making its most explicit shift.
Putting Members and Community at the Center
As part of Medi-Cal transformation, DHCS launched a two-part Health Equity Roadmap process grounded in the expressed needs of members. In 2024, DHCS conducted a statewide listening tour (11 sessions, both virtual and in person), partnering with trusted community-based organizations and tailoring sessions to specific communities.

On February 5 of this year, 65 health care and community organization leaders from across California gathered in Oakland for the latest California Improvement Network (CIN) partner meeting.
What DHCS heard was consistent and concrete: Respect is “number one.” Members described how customer service experiences shape trust, how long waits and administrative barriers block access, and how quickly trust can erode when systems feel confusing, punitive, or dismissive.
Riley underscored that the process mattered as much as the findings. Partnering with trusted community organizations was essential to creating the conditions for honest feedback. DHCS is now planning the next phase, which launches this spring, by moving from listening to codesigning actionable solutions with members, providers, plans, and community partners.
What This Means for Health and Social Organizations
Despite the current health care landscape, the state’s direction has not changed. DHCS will continue to prioritize data collection to achieve its Bold Goals, champion efforts to reduce disparities, and maintain a commitment to member engagement.
For the field, the call is steady and specific: Keep using stratified data to see who is benefiting (and who isn’t), strengthen culturally responsive practices and workforce supports, and treat member and community engagement as a core design requirement. The Bold Goals were never just a 2025 target. As DHCS continues the work, CIN partners and health and community organizations across California have a clear role to play: Use data intentionally, invest in equity-driven practice changes, deepen partnerships with community organizations, and bring lessons back to the network so others can build on them.




